Pharmacological Management

Pharmacological management of Parkinson's Disease can be fairly effective in managing some symptoms, maintaining function, preserving mobility, and enhancing quality of life (Spaulding et al., 2013). Unfortunately, over time, medications become less effective in managing symptoms with fluctuating periods of on phases and off phases (Spaulding et al., 2013). On phases of medication management are characterized by more fluid movement. Off phases can include worsening of gait, rigidity, bradykinesia, and tremor (Spaulding et al., 2013). Levodopa, a dopamine precursor, and dopamine agonists are the most commonly prescribed medications used to manage Parkinson's Disease (Spaulding et al., 2013).
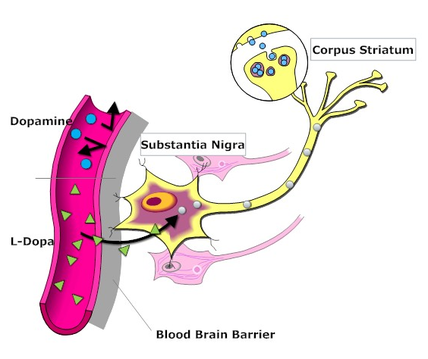
Levodopa is considered to be the gold standard in Parkinson's Disease pharmacological treatment (Sawle, 2002). It is converted to dopamine in the brain, stored and released to alleviate symptoms caused by insufficient dopamine levels (Sawle, 2002). It is more effective earlier in the disease course when there are a greater number of surviving neurons in the substantia nigra (Sawle, 2002). As Parkinson's Disease progresses, treatment becomes more difficult. Levodopa, on its own, can be broken down before reaching the brain causing side effects such as nausea and vomiting (Sawle, 2002). It is prescribed in combination with a peripheral decarboxylase inhibitor, such as Carbidopa, to inhibit side effects caused by levodopa break down in the peripheral circulation (Sawle, 2002).
Dopamine agonists can be used as an alternative to levodopa (Sawle, 2002). Symptom control may be less effective than levodopa; however, long-term side effects may be reduced (Sawle, 2002). Medication can be given to provide temporary symptom relief or can be given on a continuous basis as an alternative to other Parkinson's Disease medications (Sawle, 2002).

Monoamine oxidase inhibitors (MAOIs) can be prescribed to prolong the effect of levodopa by preventing the breakdown of dopamine (Sawle, 2002). Early in the disease course, it can slightly improve symptoms by enhancing the effect of existing dopamine. In later Parkinson's Disease, MAOIs can be used to decrease off phases and improve the continuity of pharmacological symptom management (Sawle, 2002).
Catechol-O-methyl transferase (COMT) inhibitors can be prescribed to reduce the breakdown of levodopa prior to reaching the blood-brain barrier (Sawle, 2002). More levodopa can enter the brain and be converted to dopamine, if its breakdown is prevented in the peripheral circulation (Sawle, 2002). COMT inhibitors can also enhance the effect of levodopa and improve symptom control (Sawle, 2002)
Catechol-O-methyl transferase (COMT) inhibitors can be prescribed to reduce the breakdown of levodopa prior to reaching the blood-brain barrier (Sawle, 2002). More levodopa can enter the brain and be converted to dopamine, if its breakdown is prevented in the peripheral circulation (Sawle, 2002). COMT inhibitors can also enhance the effect of levodopa and improve symptom control (Sawle, 2002)
